
Writing the greatest nursing care plan involves a step-by-step process to accurately complete all of the care plan's necessary components. For students and licensed nurses to utilise, our nursing assignment help experts have created a guide that lists the most comprehensive database and nursing care plans.
An official nursing care plan (NCP) procedure accurately identifies current needs and recognises prospective requirements or concerns. Care plans facilitate communication between nurses, their clients, and other healthcare professionals to accomplish health care results. Nurse care planning is essential to maintaining the calibre and uniformity of patient care.
A nursing care plan begins when a client is accepted to the organisation and is regularly updated when the client's health changes and goal attainment is assessed. Excellence in nursing practice is based on the planning and provision of customised or patient-centred care.
There are official and informal care plans: An internal action plan for the nurses is an informal long-term care plan. A written or digital plan that organises the client's care information is known as a formal care plan. Standardised and personalised care plans are additional divisions of formal care plans. The nursing care for clients with regular requirements is specified in standardised care plans. The special demands of a particular client that are not covered by the standardised care plan are met by individualised care plans.
The aims and goals of creating a nursing care plan are as follows:
The objectives and significance of creating a nursing care plan are as follows:
For further details, you can connect to our experts providing help in nursing assignments or childcare assignment help.
An NCP often comprises nursing diagnoses, client issues, anticipated results, nursing actions, and nursing justifications. The following details these elements:
The initial stages in creating a care plan are to examine the client's health and review any test findings and diagnostic reports. Client evaluation is specifically connected to the following traits and skills: functional, cognitive, economic, sexual, age-related, spiritual/transpersonal, psychological, cultural, and environmental. In this field, information can be both objective and subjective.
There is a list of anticipated client results. These might be both lengthy and brief.
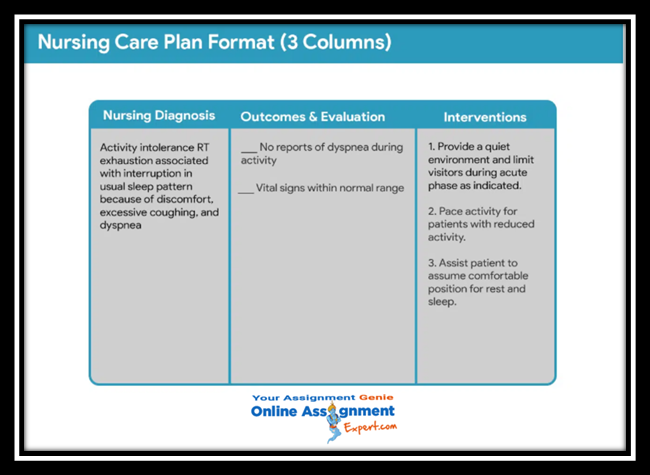
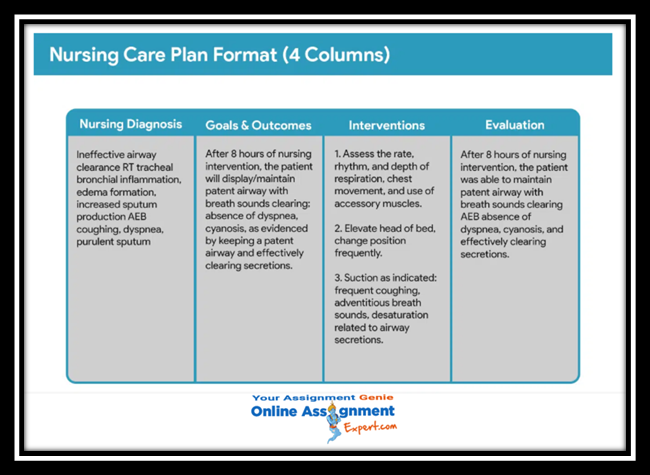
There are often four rows in nursing care planning formats: (1) nursing diagnoses, (2) intended objectives and goals, (3) nursing actions, and (4) evaluation. Goals and assessment will be in the same column in a 3 model used by certain agencies. A five-column model used by other organisations has a column for assessment cues.
As they're a learning endeavour for the student, student care plans are longer and more thorough than care plans utilised by working nurses.
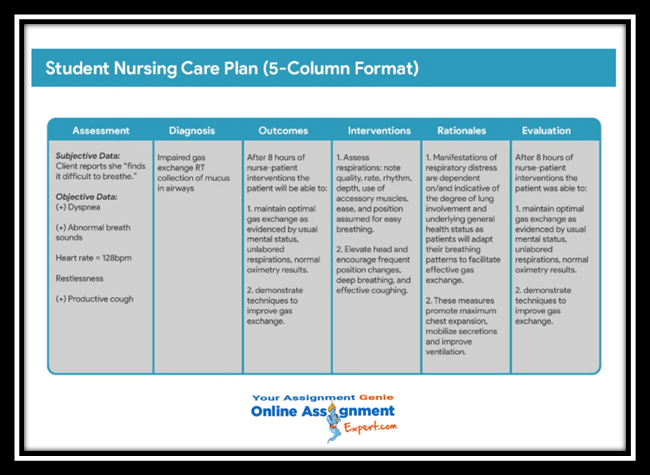
Student nurses must often write their treatment plans by hand and include a column following the nursing actions for "Rationale" or "Scientific Explanation." Science-based rational ideas provide the justifications for selecting a certain nursing intervention.
How is a nursing care plan (NCP) written? To create a care strategy for your client, simply adhere to the procedures listed below.
Using evaluation procedures and data gathering methods, a client database was developed as the first stage in designing a nursing care plan help. All obtained health data is kept in a client database. The nurse can develop a diagnosis by identifying the relevant or risk factors and describing features in this stage. You can use the unique evaluation forms some organisations or nursing schools provide.
Analyse, group, and arrange the facts to create your clinical judgment, priorities, and intended outcomes now that you know the client's health.
Using NANDA nursing diagnosis is a consistent method for recognising, concentrating on, and handling particular client requirements and answers to real, high-risk situations. Nursing diagnoses refer to actual or future health issues that can be avoided or treated without medical assistance.
Choosing a preferred order for treating nursing diagnoses and therapies is known as setting priorities. In this step, the nurse and the client start deciding which nursing diagnostic has to be addressed first. Diagnoses can be categorised and classified according to their priority as low, medium, or high. Life-threatening issues ought to be treated with extreme priority.
Maslow's Hierarchy of Needs is covered by a nursing diagnosis, which aids in planning and prioritising treatment depending on patient-centred results. Abraham Maslow created a hierarchy based on the fundamental wants that are inborn in every person in 1943. Before achieving higher wants and objectives, such as self-actualisation, and self-esteem, fundamental physiological goals and needs must be satisfied. The foundation for delivering nursing interventions and nursing care is based on safety needs and physiological needs. They are setting the groundwork for both physical and emotional wellness at the base of Maslow's pyramid.
The nurse and patient then develop goals for each priority that was decided after allocating priority for nursing assessment. Using nursing interventions based on the patient's diagnosis, the nurse aims to attain certain goals or desired results. Goals guide designing interventions, act as standards for assessing client progress, allow the client and nurse to identify which issues have been resolved, and inspire both parties by giving them a sense of accomplishment.
Each diagnosis is assigned a single overarching objective. Goal, result, and the expected result are frequently used words interchangeably.
Nursing interventions are tasks or procedures carried out by nurses to meet the needs of their patients. The suggested interventions should be directed at lowering or removing the cause of the nursing assessment. Interventions for risk nursing diagnoses should concentrate on lowering the client's health risks. Nursing interventions are chosen and documented during this stage of nursing care, but they are carried out at the time of implementation.
Rationales, often referred to as scientific justifications, describe the selection of the nursing intervention for the NCP.
Regular care plans do not provide justifications. They're included to help nursing students connect the chosen care plan with psychological and pathophysiological concepts.
The success of the NCP and the patient's progress toward goals or intended outcomes are assessed during the deliberate evaluation of continuing activities. Since the results of this stage decide if the nursing intervention should be stopped, continued, or adjusted, evaluation is a crucial part of the nursing process.
The client's treatment plan is recorded by hospital regulations and added to the client's everlasting medical file, which the ensuing nurse may review. The care plan forms vary amongst nursing programmes. The majority employ a five-column structure and are created so that the learner progressively progresses through the interconnected nursing process phases.
Hopefully, the above guide for the nursing care plan and nursing interventions will help you in your study and assignments. However, if you need something else like assignment help, feel free to reach us. We at Online Assignment Expert have assisted university scholars at different levels of their studies. Hence, share your concerns with us, and we will provide you with the best nursing assignment help.

Hi, I am Stella Adam, holding a Master’s in Educational Technology from a well-known university and currently working on innovating the educational procedures and developing digital materials for higher education (Study Material). My aim in life is to make learning more accessible, interesting and beneficial, which is why I am working as a Senior Writer with Online Assignment Expert. I have won several awards in the educational field for introducing several e-learning modules.
Get
500 Words Free
on your assignment today








